At the request of the FDA Eisai voluntarily recalled Belviq (locaserin).
01-14-2020 Initial FDA Drug Safety Communication
Safety clinical trial shows possible increased risk of cancer with weight-loss medicine Belviq, Belviq XR (lorcaserin). FDA continues to evaluate the trial results
02-13-2020 follow-up notice
FDA Requests Withdrawal of Weight-Loss Drug Belviq, Belviq XR (lorcaserin) by Eisai: Drug Safety Communication -
https://www.fda.gov/safety/medical-product-safety-information/belviq-belviq-xr-lorcaserin-eisai-drug-safety-communication-fda-requests-withdrawal-weight-loss-drug
Belviq (lorcaserin) in context
Initially the FDA was not familiar with the off label use of Belviq as an adjunctive anticonvulsant to treat intractable seizures in patients with severe epilepsy
https://n.neurology.org/content/91/18/837
It is worth noting that obesity (the condition FDA approved for treatment with locaserin, Belviq) is associated with an increased risk of cancer https://www.ncbi.nlm.nih.gov/pubmed/20507889
Diabetes, seen in many of the patients who took Belviq, is also associated with an increased risk of cancer.
https://synapse.koreamed.org/Synapse/Data/PDFData/2004DMJ/dmj-35-193.pdf
Epilepsy is not associated with an increased risk of cancer.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2077448/pdf/784.pdf
Possibly because patients with seizures avoid certain behaviors that increase the risk of both seizures and cancer such as smoking...
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3090289/
and drinking alcohol.
https://www.thelancet.com/article/S0140-6736(18)31571-X/fulltext
https://jamanetwork.com/journals/jama/fullarticle/2757730
It would be very helpful if Eisai and the FDA could make available the details of the data on which their decision to take Belviq off the market were based. The thousands of patients taking the drug for weight loss deserve to now know as much about the risks as possible. In particular how did the FDA decide that the drug should be immediately removed from the market but that cancer screening was not warranted.
To date, the single largest study (>10,000 patients) for which data is available was published in 2018 in the New England Journal of Medicine. Here there are a couple of references to cancer in table 3. There was a small risk, but it did not appear to be statistically significant, which may have been why it was not mentioned in the discussion portion of the article.
https://www.nejm.org/doi/full/10.1056/NEJMoa1808721
Knowing the risk of individual cancers associated with the use of Belviq as well as the FDA's reasons for not recommending cancer screening are particularly important for patients with epilepsy in that there is a long history of concerns about adverse effects of new antiepileptic drugs going all the way back to the 19th century and triple bromides.
When Tegretol first came on the market in 1974, it was necessary to obtain white blood cell counts every couple of weeks due to recent reports of patients dying from aplastic anemia. At the time that Depakote was approved in 1978 there was a concern about a handful of patients who had fatal hepatitis in the UK where it had been marketed for several years. Initially, frequent liver function tests were mandatory. Ulitimatley it became apparent that an at risk population (young children) could be identified and that risk greatly diminished after the first couple months on the drug. Soon after lamotrigine was approved in 1994, there was a rash of deaths from Stevens-Johnson syndrome. Again a way of mitigating the risk was found: slow titration over the first 6 weeks. Therefore, despite early problems, all three medicines ultimately proved to be safe if certain precautions were taken and all three eventually became gold standard treatments.
Sabril presented a different type of problem and for close to 15 years one had to import it from London. Ultimately monitoring with ERGs and visual field exams allowed it to be used with much less risk of visual field constriction and led in 2009 to FDA approval in the US. It has become an important niche anticonvulsant with strict FDA guidelines that initially required doctors who used it to register and submit results of visual field testing every 3 months in order to obtain the drug from one of several specialty pharmacies. The guidelines were restrictive but allowed the drug to be used safely.
Zonegran was initially developed by Warner-Lambert/Parke-Davis and Dainippon (Japan) in the 1980s but because of kidney stones seen in clinical trials (only 13 symptomatic cases in 700 patients) Warner-Lambert/Parke-Davis informed the FDA that they were no longer interested in pursuing its development in the US. In Japan Dainippon persisted and brought it on the market as Excegran where it became very popular. It was eventually FDA approved in 2000. Nephrolithias risk remains close to 2%.
Pending cancer risk data from Eisai, the example that may best parallel the story with Belviq is Felbatol, which on August 1st 1994 was withdrawn from the market because of deaths associated with its use due to aplastic anemia. Then on September 27th, the FDA
recommended that the drug remain available only for patients with severe epilepsy for whom the benefits outweighed the risks, and that changes be made to the product's labelling to reflect the newly recognized risk. This redemption came with an additional warning since there had been 10 cases acute liver failure (4 of which were fatal).
https://web.archive.org/web/20070929141432/https://www.fda.gov/bbs/topics/ANSWERS/ANS00605.html
Subsequently Felbatol has turned out to be a very useful anticonvulsant in selected patients who are willing to have their bone marrow and liver function followed closely. With time it became clear that the risk of developing these two disorders faded towards the end of the first year. It remains one of a handful of anticonvulsants not associated with significant sedation or adverse cognitive effects
In 1997 the diet drug Pondimin (combination of fenfluramine and phentermine) was withdrawn from the market because of problems with both valvular heart disease and pulmonary hypertension. Subsequently in Belgium fenfluramine was re-evaluated as a treatment for severe childhood epilepsy and shown to have efficacy at doses smaller than those used to treat obesity in adults. In light of Belviq being withdrawn from the market it is ironic that Zogenix is now trying to bring fenfluramine, which shares one mechanism of action with Belviq, back on the market.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)32500-0/fulltext
As noted above epilepsy is not a risk factor for developing cancer whereas both obesity and diabetes are. It is possible that patients with epilepsy who are not overweight and do not have diabetes may have a risk of cancer that is considerably less than those who are over weight and diabetic. And indeed as was the case with Felbatol this risk may actually be worth taking for those individuals whose quality of life has been significantly improved while using the drug, e.g. patients whose weekly convulsive seizures have been eliminated and whose families have noticed associated cognitive improvement. The risk might even be worth taking for patients with focal seizures who have been seizure free for up to a year and a half and can now safely operate a motor vehicle and discontinue drugs such as Sabril and Keppra.
Response from Dr. Janet Woodcock to a letter from the family of a patient who had a response to Belviq
From: Woodcock, Janet <Janet.Woodcock@fda.hhs.gov>
Date: Tue, Feb 18, 2020, 12:32 PM
Subject: thank you for writing.
To:
The reason Belviq was asked to withdraw is that the drug was never studied for seizure disorders and was not approved for such. I personally was not aware that it was being used for this indication. FDA will work with the firm and the community over access to the drug, we understand the benefit/risk ratio is very different for seizure disorders that are not well controlled, as compared to use in obesity to achieve modest weight loss. We also understand the time issue here.
hank you for writing. Janet Woodcock M.D.
Eisai medical information at 888-274-2378 confirms that the company is in discussions with the FDA about the use of Belviq to treat epilelpsy.
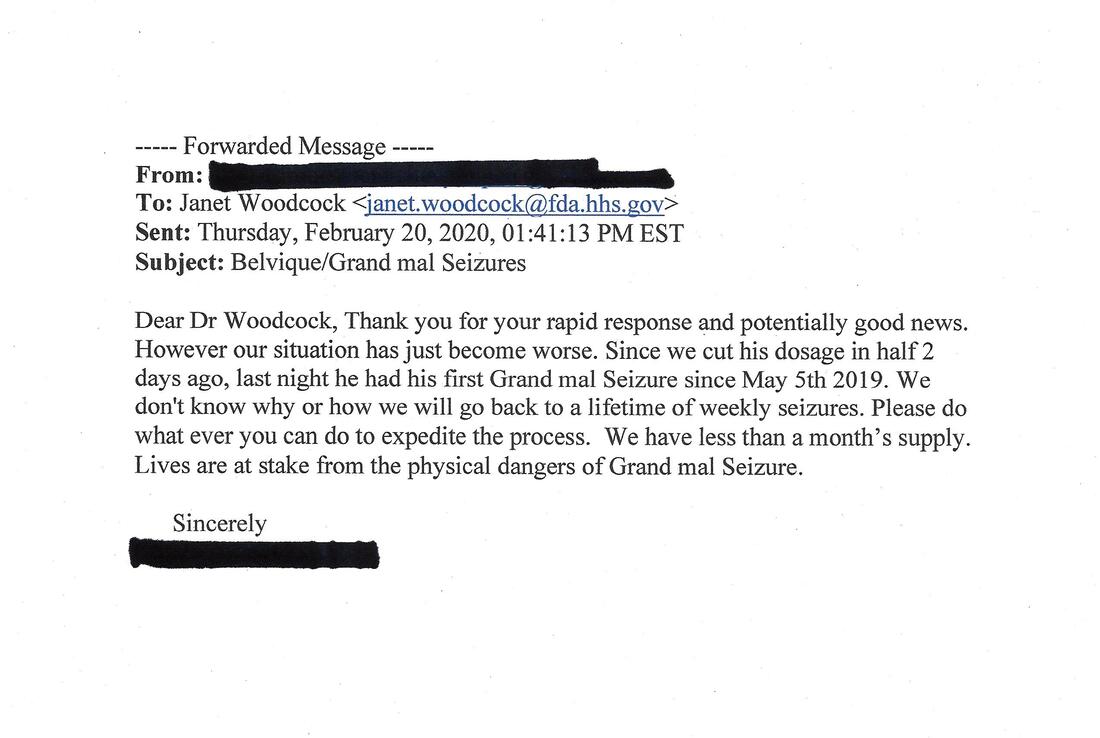
Partly in response to the letters (see below) written by patients taking Belviq to treat their seizures (and their families) Eisai and the FDA set up a compassionate use protocol whereby patients using Belviq to treat seizures at the time of its withdrawal from the market have been supplied with the drug free of charge indefinitley.
For anyone who has questions for Dr. Janet Woodcock at the FDA and would like to contact her. Note her updated email below
https://www.naabt.org/documents/Template_for_Response_Letters_to_FDA.pdf
01-14-2020 Initial FDA Drug Safety Communication
Safety clinical trial shows possible increased risk of cancer with weight-loss medicine Belviq, Belviq XR (lorcaserin). FDA continues to evaluate the trial results
02-13-2020 follow-up notice
FDA Requests Withdrawal of Weight-Loss Drug Belviq, Belviq XR (lorcaserin) by Eisai: Drug Safety Communication -
https://www.fda.gov/safety/medical-product-safety-information/belviq-belviq-xr-lorcaserin-eisai-drug-safety-communication-fda-requests-withdrawal-weight-loss-drug
Belviq (lorcaserin) in context
Initially the FDA was not familiar with the off label use of Belviq as an adjunctive anticonvulsant to treat intractable seizures in patients with severe epilepsy
https://n.neurology.org/content/91/18/837
It is worth noting that obesity (the condition FDA approved for treatment with locaserin, Belviq) is associated with an increased risk of cancer https://www.ncbi.nlm.nih.gov/pubmed/20507889
Diabetes, seen in many of the patients who took Belviq, is also associated with an increased risk of cancer.
https://synapse.koreamed.org/Synapse/Data/PDFData/2004DMJ/dmj-35-193.pdf
Epilepsy is not associated with an increased risk of cancer.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2077448/pdf/784.pdf
Possibly because patients with seizures avoid certain behaviors that increase the risk of both seizures and cancer such as smoking...
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3090289/
and drinking alcohol.
https://www.thelancet.com/article/S0140-6736(18)31571-X/fulltext
https://jamanetwork.com/journals/jama/fullarticle/2757730
It would be very helpful if Eisai and the FDA could make available the details of the data on which their decision to take Belviq off the market were based. The thousands of patients taking the drug for weight loss deserve to now know as much about the risks as possible. In particular how did the FDA decide that the drug should be immediately removed from the market but that cancer screening was not warranted.
To date, the single largest study (>10,000 patients) for which data is available was published in 2018 in the New England Journal of Medicine. Here there are a couple of references to cancer in table 3. There was a small risk, but it did not appear to be statistically significant, which may have been why it was not mentioned in the discussion portion of the article.
https://www.nejm.org/doi/full/10.1056/NEJMoa1808721
Knowing the risk of individual cancers associated with the use of Belviq as well as the FDA's reasons for not recommending cancer screening are particularly important for patients with epilepsy in that there is a long history of concerns about adverse effects of new antiepileptic drugs going all the way back to the 19th century and triple bromides.
When Tegretol first came on the market in 1974, it was necessary to obtain white blood cell counts every couple of weeks due to recent reports of patients dying from aplastic anemia. At the time that Depakote was approved in 1978 there was a concern about a handful of patients who had fatal hepatitis in the UK where it had been marketed for several years. Initially, frequent liver function tests were mandatory. Ulitimatley it became apparent that an at risk population (young children) could be identified and that risk greatly diminished after the first couple months on the drug. Soon after lamotrigine was approved in 1994, there was a rash of deaths from Stevens-Johnson syndrome. Again a way of mitigating the risk was found: slow titration over the first 6 weeks. Therefore, despite early problems, all three medicines ultimately proved to be safe if certain precautions were taken and all three eventually became gold standard treatments.
Sabril presented a different type of problem and for close to 15 years one had to import it from London. Ultimately monitoring with ERGs and visual field exams allowed it to be used with much less risk of visual field constriction and led in 2009 to FDA approval in the US. It has become an important niche anticonvulsant with strict FDA guidelines that initially required doctors who used it to register and submit results of visual field testing every 3 months in order to obtain the drug from one of several specialty pharmacies. The guidelines were restrictive but allowed the drug to be used safely.
Zonegran was initially developed by Warner-Lambert/Parke-Davis and Dainippon (Japan) in the 1980s but because of kidney stones seen in clinical trials (only 13 symptomatic cases in 700 patients) Warner-Lambert/Parke-Davis informed the FDA that they were no longer interested in pursuing its development in the US. In Japan Dainippon persisted and brought it on the market as Excegran where it became very popular. It was eventually FDA approved in 2000. Nephrolithias risk remains close to 2%.
Pending cancer risk data from Eisai, the example that may best parallel the story with Belviq is Felbatol, which on August 1st 1994 was withdrawn from the market because of deaths associated with its use due to aplastic anemia. Then on September 27th, the FDA
recommended that the drug remain available only for patients with severe epilepsy for whom the benefits outweighed the risks, and that changes be made to the product's labelling to reflect the newly recognized risk. This redemption came with an additional warning since there had been 10 cases acute liver failure (4 of which were fatal).
https://web.archive.org/web/20070929141432/https://www.fda.gov/bbs/topics/ANSWERS/ANS00605.html
Subsequently Felbatol has turned out to be a very useful anticonvulsant in selected patients who are willing to have their bone marrow and liver function followed closely. With time it became clear that the risk of developing these two disorders faded towards the end of the first year. It remains one of a handful of anticonvulsants not associated with significant sedation or adverse cognitive effects
In 1997 the diet drug Pondimin (combination of fenfluramine and phentermine) was withdrawn from the market because of problems with both valvular heart disease and pulmonary hypertension. Subsequently in Belgium fenfluramine was re-evaluated as a treatment for severe childhood epilepsy and shown to have efficacy at doses smaller than those used to treat obesity in adults. In light of Belviq being withdrawn from the market it is ironic that Zogenix is now trying to bring fenfluramine, which shares one mechanism of action with Belviq, back on the market.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)32500-0/fulltext
As noted above epilepsy is not a risk factor for developing cancer whereas both obesity and diabetes are. It is possible that patients with epilepsy who are not overweight and do not have diabetes may have a risk of cancer that is considerably less than those who are over weight and diabetic. And indeed as was the case with Felbatol this risk may actually be worth taking for those individuals whose quality of life has been significantly improved while using the drug, e.g. patients whose weekly convulsive seizures have been eliminated and whose families have noticed associated cognitive improvement. The risk might even be worth taking for patients with focal seizures who have been seizure free for up to a year and a half and can now safely operate a motor vehicle and discontinue drugs such as Sabril and Keppra.
Response from Dr. Janet Woodcock to a letter from the family of a patient who had a response to Belviq
From: Woodcock, Janet <Janet.Woodcock@fda.hhs.gov>
Date: Tue, Feb 18, 2020, 12:32 PM
Subject: thank you for writing.
To:
The reason Belviq was asked to withdraw is that the drug was never studied for seizure disorders and was not approved for such. I personally was not aware that it was being used for this indication. FDA will work with the firm and the community over access to the drug, we understand the benefit/risk ratio is very different for seizure disorders that are not well controlled, as compared to use in obesity to achieve modest weight loss. We also understand the time issue here.
hank you for writing. Janet Woodcock M.D.
Eisai medical information at 888-274-2378 confirms that the company is in discussions with the FDA about the use of Belviq to treat epilelpsy.
Partly in response to the letters (see below) written by patients taking Belviq to treat their seizures (and their families) Eisai and the FDA set up a compassionate use protocol whereby patients using Belviq to treat seizures at the time of its withdrawal from the market have been supplied with the drug free of charge indefinitley.
For anyone who has questions for Dr. Janet Woodcock at the FDA and would like to contact her. Note her updated email below
https://www.naabt.org/documents/Template_for_Response_Letters_to_FDA.pdf